
The Bayh-Dole Coalition recently posted on Twitter a claim that the development of the nicotine patch was a Bayh-Dole “success story”:
Bayh-Dole Success Story! Did you know that the nicotine patch was developed at @UCLA and commercialized via Bayh-Dole? Check out this inspiring story of scientific research helping millions kick their smoking habit from @AUTM’s Better World Project! buff.ly/33CGxvZ
Well, it’s true that the link provided connects to a “story.” And AUTM did publish the story as part of its Better World Project. And it is also true that the rights to at least two versions of the nicotine patch did claim to go “via” Bayh-Dole. But on the main points, AUTM has it wrong, and BDC uncritically repeats AUTM. They are both wrong, and their “story” misleads.
To save you lots of time, I’ll summarize:
(1) The UC nicotine patch “invention” was not a subject invention under Bayh-Dole. A court examined the evidence and ruled it wasn’t Bayh-Dole.
(2) Ciba-Geigy took an exclusive license and used the UC patent to sue Alza Corporation to prevent it from getting its nicotine patch to market first. A court later ruled that most of the UC patent claims that mattered were invalid.
(3) Meanwhile, UC used its (not-yet-invalidated) patent to create an interference in the USPTO to challenge a patent for a nicotine patch invented at New Mexico Tech. UC got a number of NMT’s patent claims invalidated based on UC’s claim of prior invention.
(4) As a result, UC also used its patent position to leverage a share of NMT’s royalty income–on NMT’s patent also licensed to Ciba-Geigy. That fight cost UC and NMT Research Foundation, collectively, over a million dollars in legal fees.
(5) The UC nicotine patch invention was one of many–hundreds, by the time UC filed–patented inventions in the area of transdermal drug delivery. UC’s inventors were chasing a hot area of industry activity, and got there relatively late with a minor bit of improvement, mostly not patentable.
(6) Turns out that nicotine patches are not all that effective. At six months there’s no difference between the patch and going cold turkey. UC should never have allowed its inventors to run clinical trials at UC.
(7) The UC inventors argued for nicotine replacement therapy based on the idea that nicotine is the addictive element in smoking. Studies now suggest that nicotine–one of multiple forms of nicotine-like compounds found in cigarettes–is not the addictive element. A mystery for real science. But UC pushed commercial marketing before the science got done.
In all, nothing about Bayh-Dole has been a net positive for nicotine patches. We might say, rather, that nicotine patches have survived attacks by people wielding inventions controlled under a claim of Bayh-Dole. Telling the story shows how patents get used in the real world–and shows that neither the Association of University Technology Managers nor the Bayh-Dole Coalition has a freaking clue what it is talking about in calling UC’s nicotine patch a success. Shall we?’
The idea to use nicotine to help tobacco users quit goes back a long way. In 1907, Carleton Ellis obtained a US patent (865,026) for a “masticable tobacco preparation“–yes, nicotine gum–as an alternative to chewing tobacco. Ellis never made a product of it (he was busy inventing margarine, among other things), but his patent presents a number of ideas basic to nicotine replacement therapy: use nicotine, get it absorbed into the body, and bingo. In the early 1960s, Ove Frenö, the director of research at Atiebolaget Leo, a Swedish pharmaceutical firm, developed Nicorette gum to do just what Ellis had imagined. Leo obtained a US patent in 1974 (3,845,217).The history of transdermal nicotine patches, then, takes place in the context of a longer history of transmucosal nicotine therapy.
Pastore, et al. trace the development of transdermal patches in “Transdermal patches: history, development and pharmacology.” While the idea of applying medicines to the skin to achieve a clinical effect goes back to 3000 BC, the stuff we are interested in begins with the work of Dale Wurster and Sherman Kramer in the early 1960s. That would be the system identified as “G” in this figure from Pastore, et al.: 
The idea that nicotine could be absorbed through contact with the skin was documented in the 1930s. What was missing was combining all this into a working patch system involving nicotine and an adhesive. From there it is a matter of how to store the nicotine in the patch, what materials might be used for that purpose, and how the components are configured. Will the nicotine be liquid or a gel or an ointment? What sort of dose to deliver, rate controllers for the dose, and skin conditioners to aid absorption and the like? In other words, there’s lots of variation possible for any given patch system, some of it obvious and some of it less so. Wurster and Kramer worked with salicylates, not nicotine, but they appear to be first with the overall concept. As Pastore et al. puts it, their system “appears very much to be the forerunner of cells currently used in transdermal research and could even be considered a first prototype of today’s commercial transdermal devices.”
Around the same time, Raymond Osbourn and Thomas Tusing at Hazelton Laboratories filed a patent application on June 22, 1962 for “Sensitivity Test Patches,” consisting of an outer casing and a pad into which various agents can be introduced and then the patch is placed on the skin to determine whether the skin is sensitive to those agents. In a sense, Osbourn and Tusing’s patch delivers all sorts of things into the skin. Their purpose was diagnostic rather than therapeutic. For therapeutic uses, we turn next to Alza Corporation.
In April 1969 Alejandro Zaffaroni filed a patent application for a “bandage” that delivered “continuous administration of systemically active drugs by absorption through the skin or oral mucosa.” The patent issued in 1971 (3,598,122). There’s the basic idea of a patch that can deliver most anything. Yes, it could deliver even nicotine–as many people realized, but mostly a decade later. Zaffaroni assigned his patent to Alza Corporation, the company he had founded in 1968. Alza became a major player in the development of patch technology, passing briefly into the control of Ciba-Geigy via a research agreement that gave Ciba-Geigy substantial control over Alza from 1977 to 1981. Zaffaroni received a number of subsequent patents related to patch technology (all assigned to Alza), including 3,996,934, 5,071,656, and 5,284,660 (filed 1988, issued 1994, claiming nicotine). Alza’s first product was “Transderm Scop” in 1981, using scopolamine to treat nausea. In 1990 the FDA approved Duragesic, delivering fetanyl for cancer pain. And in 1991, Alza’s Nicoderm patch was the first approved by the FDA.
One might say, generally, that Zaffaroni developed the commercial idea of a transdermal patch delivering any of various therapeutic agents, and his company brought products to market, evidencing the capability of its systems. Alza, then, as it were, invented the transdermal patch as a commercial item. And invented a patch with nicotine–just it was not first to stake a patent claim to the use of nicotine in a patch.
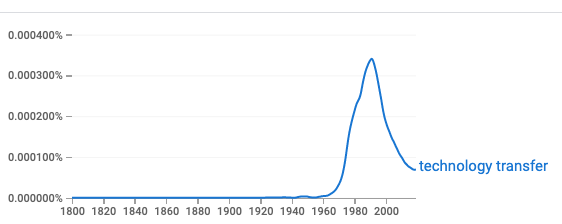
And all this work was done without federal funding. There was also no particular need for “technology transfer” from a university as Alza did its own inventing and development. Indeed, the concept of “technology transfer” is largely bureaucratic in origin, in the U.S. arising, it appears, in the mid-1960s as an organizing principle used by federal agencies to explain how they were to respond to Vannevar Bush’s call to “lift the lid” on classified science and technology developed during the second world war. Here’s an ngram view of “technology transfer” as a proxy for frequency of use:
See for instance the first chapter in Technology Transfer and Innovation: A Guide to the Literature, 1966.
Today there is a great deal of new technology in search of a demand. The following programs are major efforts of the Federal agencies [DoD, NASA, and AEC, accounting for 90% of federal research and development expenditures] to select, evaluate, interpret and disseminate new technology in order to find a place for it in the civilian economy. (9)
Alza was decades ahead of UC’s activities pertaining to patches. By the time UC filed its patent application for a nicotine patch in April 1985, Alza had obtained over 300 U.S. patents with a priority date earlier than UC for many different variations on the theme of delivering medicines involving some sort of patch applied to skin, mucosa, anus, uterus, eye, and ear. There were both general patents as well as patents that identified specific compounds. Alza just didn’t get around to calling out nicotine in a patent application until July 14, 1988–four years after UC had filed its patent application. Similarly, Hercon Laboratories had five issued patents (with application priority to September 1982) on transdermal systems to deliver nicotine–among other drugs–before UC filed its patent application. American Home Products had a pending patent application for a transdermal patch dating from December 1983, with a continuation-in-part application April 1987 (a standard “submarine” patent, pre-reform) and surfacing as an issued patent in June 1990.
But by then–April 1985–one would think that merely adding nicotine to a transdermal patch would be obvious–anyone could see how to do it, if one cared to do it, using only ordinary skill. Any inventive activity then would necessarily concern unexpected things about nicotine, nicotine-like compounds, and compounds that assist in the absorption of nicotine (or other compounds) into the bloodstream how the body deals with what gets absorbed, or improved patch composition or design, or dosing in an unanticipated way to achieve a particular purpose, such as quitting smoking permanently.